
Ring, Ring: The eDoctor is In!

Taking advantage of a world of increasing digitalization, Teladoc is disrupting the healthcare space by providing customers access to doctors 24/7 right from their home.
Imagine waking up with the familiar body aches, chills, and fever of the flu. You have to get dressed, trudge to the doctor, and wait in the waiting room – only to have the doctor spend a few minutes with you. Now imagine a different situation. Instead of leaving the comfort of your bed, you have access to a doctor within minutes from your smartphone or tablet. This is the world Teladoc is attempting to create.
The Current Healthcare Crisis
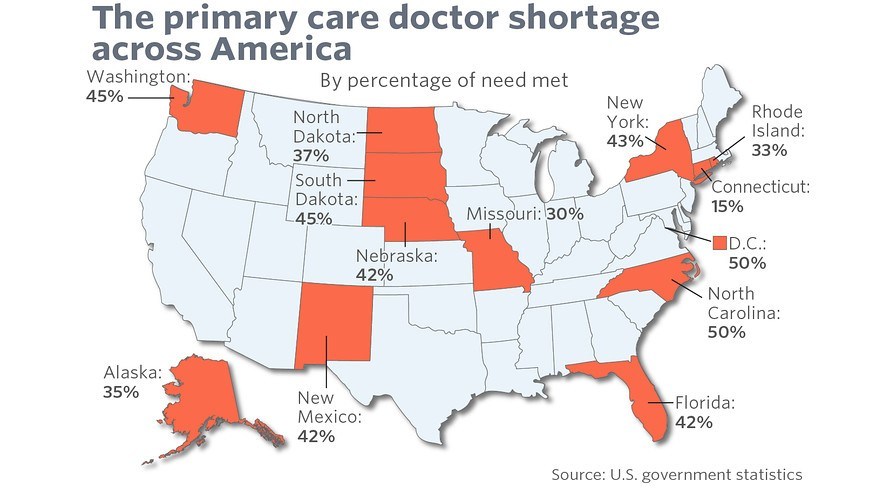
The U.S. healthcare system is broken. As of 2014, U.S. healthcare spending had reached $3.0 trillion per year and accounted for 17.5% of GDP.1 Additionally, the system has been struggling to adapt from a fee-for-service system to a value-based care system. Lastly, demand for healthcare practitioners outstrips supply, particularly for primary care physicians.2
Teladoc’s Business Model: Disrupting the Market

Teladoc was founded in 2002 to tackle these three issues within the healthcare industry: timely access to healthcare practitioners, the rising cost of healthcare, and quality of doctors and a patient’s experience.3 Teladoc provides patients with 24/7/365 access to board-certified physicians via Teladoc’s technology platform that can be accessed on a computer, tablet, or smartphone. These doctors can see a patient within minutes and can even prescribe prescriptions for common conditions. Not only does this model benefit the patient, but it also helps decrease overall costs for treatment by triaging patients to an overall lower cost of care environment. The video below gives a glimpse into the Teladoc model.
https://www.youtube.com/watch?v=8Zl7oqokjNo
Teladoc’s Operating Model
To deliver on the customer promise of high-quality, low-cost, and timely access, Teladoc has adopted a unique operating model.
- Teladoc’s Customers – Lowering Cost of Care: Teladoc’s targeted customers are large employers and payors, who can offer the service to their plan subscribers. Teladoc monetizes its business by charging both a PMPM (per member per month) fee to the plan sponsor and an additional fee when a patient utilizes Teladoc. Despite the double-fee structure, given the low cost of Teladoc’s services compared to traditional healthcare providers, plan sponsors can save significantly. To date, Teladoc has taken $600 million of costs out of the healthcare system.4
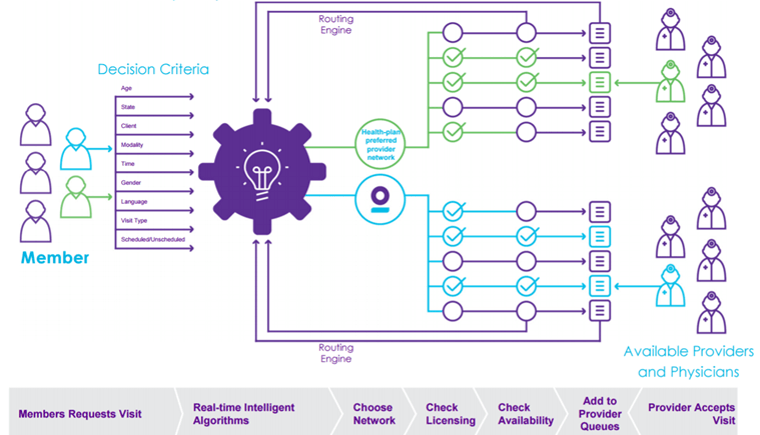
- Teladoc’s Technology – Fixing Access Issues: Teladoc addresses the issues regarding access through its technology platform. Patients can request an appointment ahead of time or be instantly rerouted to an on-demand appointment.5 Furthermore, Teladoc’s technology is scalable and able to accommodate 100M members.4 Teladoc’s algorithmic platform is shown below.5
- Teladoc’s Employees – Addressing Quality of Care: Teladoc does not employ any full-time physicians; rather, it makes use of excess capacity of already practicing physicians, such as hours outside of clinic hours and physicians working part-time schedules. Teladoc also tries to address the perception of quality in terms of the amount of time spent with the patient, averaging 6.5 minutes per patient.4 Lastly, Teladoc has received two years of consecutive perfect certifications (2014 and 2015) from the National Committee for Quality Assurance.6 Clearly these measures have been successful as Teladoc has had no reported quality issues since its inception.4
Additional Steps
Teladoc has made significant strides as the first player in the telemedicine space, adding services for behavioral health, dermatology, and tobacco cessation. Teladoc has grown to 17 million members and over 3,000 visits a day.4 However, why Teladoc has not caused as significant a disruption in healthcare is simple: a lack of awareness.
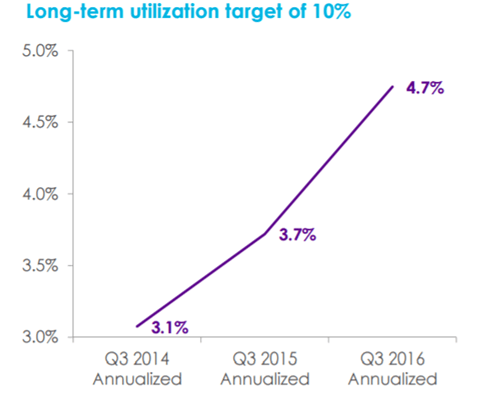
As shown below, utilization rates have been below 5% of those who have access to Teladoc.5 This low utilization rate has caused Teladoc to lose clients, including Highmark’s fully-insured clients.7
To address this issue, Teladoc has instituted welcome kits and targeted marketing on social media and smartphones for organizations that have subscribed to Teladoc.5 However, I think more needs to be done to encourage usage.
- Eliminate Legislative Barriers: One key barrier to telemedicine is legislation – only certain states allow telemedicine providers to prescribe prescriptions. Without this ability, the use of telemedicine is limited.4 Teladoc should continue to campaign to extend the reach of telemedicine.
- Generate Consumer Awareness of Cost: Given the differential in cost between a telemedicine visit and a visit to an urgent care or primary care doctor, Teladoc can impact a patient personally – namely in his wallet. One potential idea would be to partner with the health insurer or plan sponsor to include on a patient’s bill what the cost would have been had he utilized Teladoc instead.
- Profit Sharing: The last thing Teladoc could consider is changing its revenue model to mimic the healthcare industry, moving from a fee-for-service to value-based. Instead of charging a flat fee for access to Teladoc, it could move to charging a higher fee to the insurer when the service is used. This would align incentives across Teladoc and the insurer.
Word Count: 791
Sources:
- “NationalHealthAccountsHistorical.” Center for Medicare and Medicaid Services, n.d. Web. 11 Nov. 2016.
- Court, Emma. “America’s Facing a Shortage of Primary-care Doctors.” N.p., 04 Apr. 2016. Web. 11 Nov. 2016.
- “About Our Company.” – Teladoc for Members. N.p., n.d. Web. 11 Nov. 2016.
- Gorevic, Jason. “Teladoc: Keynote Speech.” HBS Healthcare Alumni Association 2016 Conference. Charles Hotel, Cambridge. 11 Nov. 2016. Lecture.
- “Teladoc Quarterly Investor Presentation.” Teladoc Quarterly Investor Presentation. Web. 11 Nov. 2016. <http://s21.q4cdn.com/672268105/files/doc_presentations/2016/TDOC-Presentation-10-25-16.vUploaded.pdf>.
- “Teladoc Receives NCQA Recertification – Press.” Teladoc Receives NCQA Recertification – Press. Teladoc, 26 June 2015. Web. 11 Nov. 2016.
- Comstock, Jonah. “Teladoc Loses $1.5M Highmark Contract, Sparks Debate on Pricing, Utilization of Telemedicine.” MobiHealthNews. N.p., 01 Dec. 2015. Web. 11 Nov. 2016. <http://www.mobihealthnews.com/47345/teladoc-loses-1-5m-highmark-contract-sparks-debate-on-pricing-utilization-of-telemedicine>.
- Cover Image: Doctor with iPad. Digital image. Telemedicine: What Should You Know? Solix, 30 June 2016. Web. 12 Nov. 2016. <http://www.solixinc.com/2016/06/30/telemedicine-what-you-should-know/>.
Very impressive business with disruptive innovation. Personally I have been living abroad for a few years and the healthcare systems in different countries always create confusion to me. On the one hand it is not very easy to see a doctor when I discover symptoms. Normally I will have to go through a tedious appointment system. On the other hand going to clinic and seeing a doctor there is usually not a great experience. Therefore, I am very impressed by Teladoc’s business model and I wish that it would scale up quickly.
Great post, Kelly! This seems almost too good to be true! I think that the issue of growth may also involve a level of trust, in addition to the awareness. I’m not sure that I would trust the opinion of a doctor that I talked to via an app who wasn’t able to physically examine me. For example, how can the doctor tell if you have an ear infection without physically looking in your ear? In addition, it seems dangerous to to prescribe a prescription without having examined the patient. I am surprised that it is legal to prescribe a prescription without physically examining the patient. I love the operating model, but think they need to not only increase awareness but also gain the trust of the customer.
Kelly – great post on Teladoc! I really enjoyed reading about the way the business model works, I had no idea that they didn’t have their own doctors but rather pulled on the excess capacity of other physicians.
As great as this model sounds in theory, I think some of the barriers you listed are insurmountable. I had Teladoc as a service through my employee benefits at my last job and I ultimately never used them for two key reasons:
1) When I thought (and actually did) have strep throat, I wanted to use Teladoc services and couldn’t. If I had called Teladoc, the doctors wouldn’t have been able to do anything for me since they could not prescribe antibiotics at that time in my state. So ultimately when I was most desperate for immediate care, these services could not work for me.
2) While I am luckily healthy and have no pre-exisiting conditions, I wonder how Teladoc will work for others who are not in the same boat. Getting Teladoc your previous medical records would be extremly challenging due to HIPAA regulations. I know this is a problem other healthcare start-ups face, like ZocDoc – but in ZocDoc’s case, patients can bring their physical medical records with them to the physician’s office who they have never seen before. Has Teladoc done anything to figure out how past medical records can be shared with physicians treating patients virtually?
Great post on Teladoc, Kelly. I find the business model really interesting.
Every time I am down with the flu, my family general practitioner (“GP”, the equivalent of a primary care physician in the USA) would always prescribe me the same medications. As a kid, I used to think the job of a GP must be really easy, by simply matching the ailments with the respective drugs. It was only more recently that I realized that the role of the general practitioner is not just to dish out the same prescriptions everyday.
The value-add of the GP (and his/her multiple years of medical training) is in picking out the esoteric medical conditions during regular consultations for flu and stomach upsets. This requires both history taking and a physical examination (as pointed out by Maria as well). Teladoc is clearly still lacking the physical examination component, which makes it inferior to a GP. It would definitely be amazing if telemedicine can be further enhanced to include this physical examination component in the near future.
Kelly, many thanks for sharing your knowledge about this industry. The article certainly brought up many thoughts for me about an industry I am not too familiar with. As Amelia mentioned, I always thought the role of a General Practitioner (GP) or Primary Care Physician (PCP) was not too tedious when I was younger, but my thoughts have certainly changed as time has progressed.
I have listed out my biggest concerns about Teladoc below and welcome your thoughts.
1) The thought of using excess capacity to address patients reminded me of Uber and Airbnb because of the sharing economy model; however, as we have seen in our cases and in industry, the sharing economy is not always accepted by all. How do physicians feel about the model, and how do they benefit by become participants in it?
2) Do you think this model of sharing idle resources can be replicated across other areas of the medical industry? I immediately began to think about pharmacies that may not see the influxes of demand that others experience. Therefore, pharmacies that have excess capacity could fill orders for patients, but may need to compete on price.
3) Would PCP or GPs be rated by patients? This may create higher demand for some practitioners versus others, creating the spikes in demand that exist today.
The healthcare industry is one that requires constant evolution to help reduce costs and to overcome the barriers of limited supply. It would be great to see Teledoc succeed in this arena.
Thanks for shedding some light on this incredibly relevant topic Kelly! I think that the trend in healthcare is indeed towards leveraging technology more and more to connect patients with providers. Like the commenters above me though, I have some concerns around Teladoc’s operating model. The inability to collect vitals and perform a physical exam is concerning to me from a provider perspective. To run with Lindsey’s example of strep throat, current best practice guidelines recommend that physicians calculate a score to determine the likelihood of strep, and 3/5 parts of that score require a physical exam. If the patient’s score suggested that they are likely to have strep, the provider would then administer a rapid strep test before giving antibiotics – so really none of this could be done through Teladoc (at least in accordance with current guidelines). I would also be concerned that Teladoc’s operating model lends itself to physicians overprescribing antibiotics, which is harmful from a societal standpoint as it contributes to the rise of multi-drug resistant bacteria. Most of the diagnoses mentioned in the video would from my perspective be best addressed in an urgent care setting, so I think the solution is to make urgent care more affordable, in part by leveraging lower cost health providers such as NPs and PAs who are more than qualified to treat colds, allergies, etc.