
Aravind Eye Care’s Grand Vision for India
Can quality and affordability go hand-in-hand for healthcare services? Aravind Eye Care is determined to make this a reality!
![]()
Healthcare systems around the world are plagued with the challenge of balancing quality and affordability. Aravind Eye Care has embraced the challenge and is revolutionizing the vision care system in India by providing high quality care at low costs. It’s business model focuses on achieving this goal leveraging economies of scale, cross subsidisation and vertical integration.
Founded in 1976, Aravind’s non-profit network – consisting of five hospitals, a research institute, an intraocular lens factory, an eye bank and – is currently the largest and most productive eye-care service group in the world.
Table 1: Key Performance Metrics
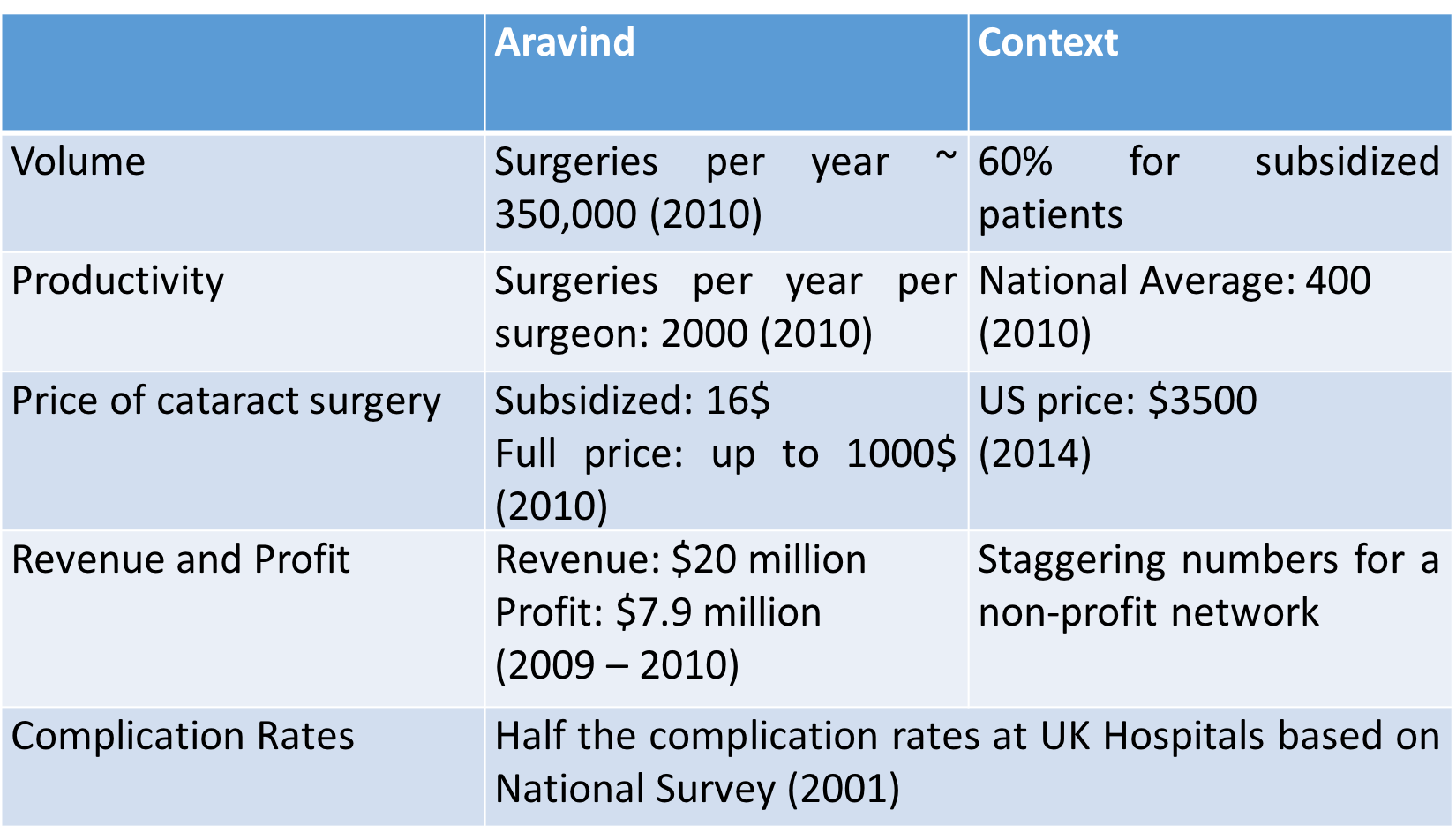

Key Features of Operating Model
- Differential Pricing for equitable treatment
As indicated in Table 1, differential pricing is an important feature of Aravind’s model. The full price paid by one well-off patient funds the treatment for several poor patients.
The quality of treatment however remains the same across patients ensuring that complication rates match global standards. The only difference is in the type of lens used and the quality of post-surgery amenities provided. While a subsidised patient is provided a basic hard lens and room on a sharing basis, patients paying the full price can choose from an array of options.
Cross subsidisation is only sustainable if the costs of the hospital are low.
- Lowering fixed costs
Fixed costs – infrastructure, equipment and salaries – are the main driver of costs for any health care system.
2.1 Utilization and Productivity
Aravind is focused on maximizing the utilization of its infrastructure and equipment and increasing the productivity of its workforce. It ensures that doctors are focused only on the critical tasks of diagnosis and surgery. By providing high-quality training and standardizing procedures, it equips nurses to take care of several non-surgical tasks.
An of-cited example is the use of the just-in-time approach to increase the utilization of its operating rooms. A typical room at Aravind has two operating tables and several other equipment to perform non-surgical tasks. When a doctor is operating on one patient, the nurse performs non-surgical tasks on the other patient. As soon as the doctor finishes with the first patient he/she can move the surgical set up to the other patient and start the next procedure.
2.2 High-volume of patients
Large patient volumes are critical to spreading fixed costs and gaining bargaining leverage with equipment suppliers. Given the non-life threatening nature of vision problems, surgical eye-care is deprioritized in large parts of India. As a consequence, India is home to almost one-quarter of the world’s blind population.
Beyond its hospitals, Aravind uses a three-pronged approach – community clinics, tele-medicine centers, eye camps – to increase access to preventive eye-care, to increase awareness about surgical eye-care and to direct willing patients to Aravind hospitals. The community benefits by gaining access to basic eye-care at their doorstep and the hospital is able to increase its volume of patients.
- Lowering variable costs
Identifying the high price of intraocular lenses (~ $70) as an impediment to its goals, Aravind set up Aurolabs in 1992 to manufacture its own lenses.
Since 1992 Aurolabs has
- Designed a manufacturing process that reduces the price of lenses to $2
- Become a global supplier of intraocular lenses
- Encouraged other players to produce low-cost, high quality lenses
- Training and Research
Training institutes are another form of vertical integration that allow Aravind to have a pipeline of well trained doctors and nurses.
Nurses and technicians, comprising 60% of the workforce, are the backbone of it’s operating model. Every year Aravind identifies women from local communities and provides them advanced training to become nurses. Aravind also offers a two-year post-graduation specialisation in ophthalmology and recruits over 45 doctors annually from the institute.
A strong performance monitoring system and a focus on research ensure that these doctors and nurses continue to innovate and excel.
Aravind has invested several years in developing a robust operating model that is well aligned to deliver high quality care at low costs and serves as a shining example of the potential of compassionate capitalism.
References:
- http://www.aravind.org/
- Health International (2011), “Driving down the costs of high-quality care: Lessons from the Aravind Eye Care System”, McKinsey’s Health Systems and Services Practice
- Forbes (2010), “Aravind Eye Care’s Vision for India”, Naazneen Karmali,
Link: http://www.forbes.com/global/2010/0315/companies-india-madurai-blindness-nam-familys-vision.html
- http://www.allaboutvision.com/conditions/cataract-surgery-cost.htm
Thanks for providing a summarized view of Aravind Eye Care, Abhilasha. I have always been intrigued by the idea of providing affordable, high-quality healthcare. One concern I have with this model though is how to ensure high quality in such an intense environment where productivity has to be maximized. I am not sure if I would like to be operated on (esp. on my eye) by doctors and nurses who have been in back-to-back surgeries for many hours.
Just curious if you have any perspective on how Aravind takes care of this.
Thats a great question Mohit. But it’s worth noting that the doctors and the support staff aren’t actually working longer hours than their peers in other hospitals. Rather the hospital has made an effort to ensure that each member performs the most value adding task – doctors only focus on diagnosis and surgery and don’t have to spend time on other pre-surgical tasks. Thus they are using their time more effectively while still working similar hours. This couples with a strong performance management system creates a good mechanism for addressing the concerns you have raised and ensuring that their complication rate matches global standards.
Very interesting case: Reminded me of our first HBS case on Narayana Hrudayalaya ! Very interesting to see how the tools and concepts like Just In Time that we have seen in the industrial or electronic industries (e.g. Toyota) in TOM apply to healthcare providers. I am wondering if this model could be exported to developed countries in a viable way ?