
Emergency Now!

Receive care promptly, and smooth demand.



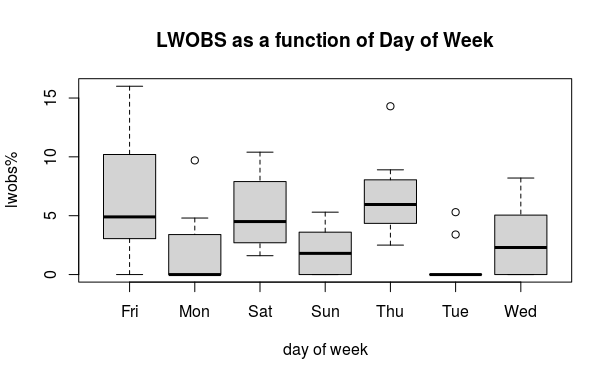
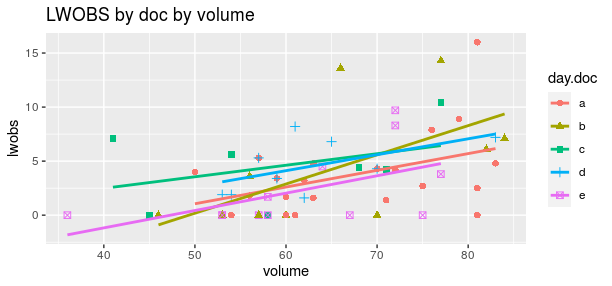
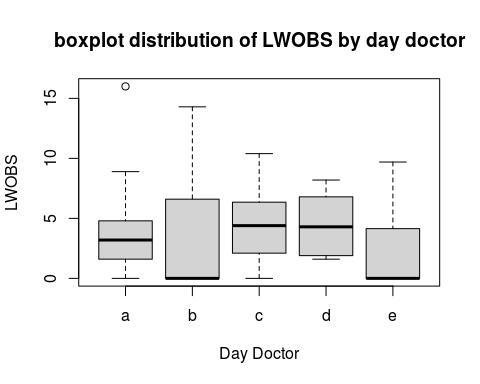
Examples of data obtained from the EMR that will contribute to the platform’s analysis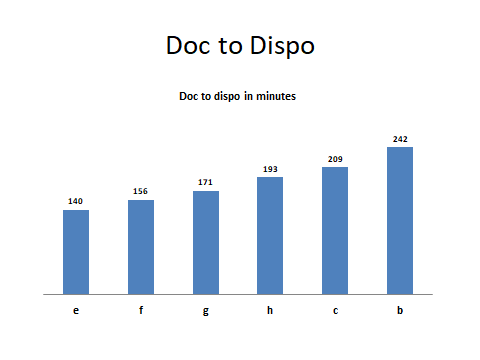
-
- Vision and value proposition: Provide real time demand data to consumers of urgent healthcare to aide in patient planning and smooth facility demand.
- The problem: Generally acutely ill or injured patients have no information about wait times as they make make the healthcare decision to present to an emergency department or urgent care facility. Patients arrive to find the waiting room full and their wait times to be both opaque and excessive. A person arriving with chest pain may then elect to go back home instead of seeking care convincing themselves that they just pulled a muscle. Conversely emergency departments and urgent cares staff for average demand but are often met with surge demand that overwhelms their systems our lack of demand that leaves valuable resources idle.
- Target market and opportunity: The market is both B2B and B2C. The B2B market are all emergency departments and urgent care facilities in the United States. There are currently about 5200 emergency departments in America and about 9000 urgent cares making the total market opportunity around 14,000 facilities. Capturing a quarter of this market yields 3500 facilities give or take 1000 (95% confidence interval). Using a subscription model and pricing this modestly at $1000 a month provides a revenue estimate of 30 million to 54 million dollars annually. The B2C model addresses around 150 million visits annually to emergency departments and about 160 million visits to urgent cares. This market therefore represents about 300 million opportunities. If 20% of this could be captured that represents a 60 million visit opportunity give or take 20 million (95% confidence interval). To abolish barriers to entry no fee or advertising will be allowed initially, in fact incentives will be provided to generate participation.
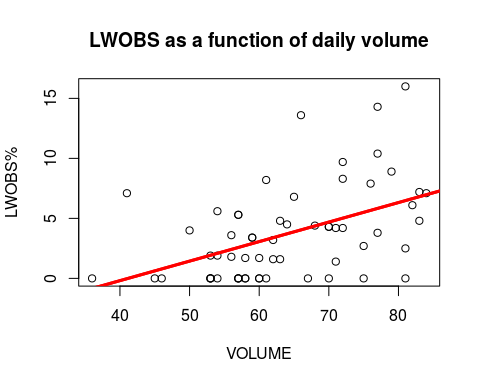
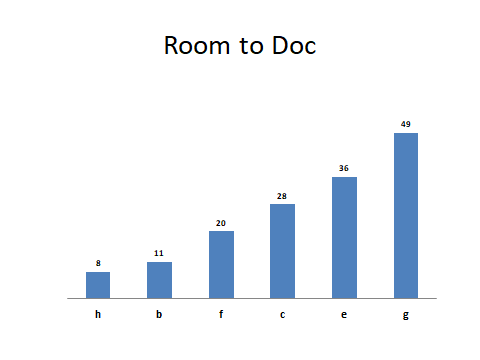
- The solution: Demand in the emergency department and urgent care setting is characterized by surges that do not neatly follow a predictable pattern. Staffing levels are planned through gut feeling, bench marking services, or by average demand. These staffing patterns are not particularly dynamic. Providing an analytic platform accessed by the public via a smart phone app can smooth out demand. For example a mother of three at home with febrile coughing children can access the app and see that currently there is a 3 hour wait for care but 2 hours from now that wait is predicted to be 45 minutes. With that information she can medicate her children at home and pack them up for their visit to the urgent care 2 hours hence. This provides convenience to the patient and allows for smoother demand for the facility. Using forecasting, queuing theory, basic statistical tools, and the electronic medical record (EMR) database along with machine learning this platform can predict demand and through a feedback loop learn to improve it’s forecasting. Elements of the EMR database that will be useful in forecasting are the characteristics of the individual providers (their unique service rates (mu) and their number (c)), the nursing and ancillary staff and services characteristics, current demand (lambda), the acuity of the current demand, and special community events that influence demand.
- Team: The team currently consists of me Miles Nelson, MD, MBA and Judith Bassik. I am an emergency physician an entrepreneur and a (soon) data analyst. Judith is a healthcare consultant and a (soon) data analyst. Key positions that need to be filled are for a coder, a statistician, and platform and app developer, a marketer, and some form of adult supervision.
- Competition: I am unaware of any competing solution.
- Images and visuals:

